
Last Updated on 13/07/2026
Written by: Dr. James Anderson, PharmD, BCPS
Department of Pharmacy Practice, Faculty of Medical and Health Sciences
Medically reviewed by: Dr. Leon Charles, PhD, ABPP-CN, Dr. Dave Lewis, MD, PhD
Abstract
Background
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental condition affecting approximately 5% of children and adolescents worldwide, with symptoms persisting into adulthood in up to 70% of cases. While psychostimulants (methylphenidate and amphetamines) remain first-line pharmacotherapy, concerns regarding adverse effects, abuse potential, and tolerability have driven interest in alternative agents. Modafinil a wakefulness-promoting agent with a unique “atypical” central nervous system stimulant profile, has emerged as a candidate for off-label ADHD management.
Objective
This systematic review synthesises the current evidence base for modafinil in ADHD, examining its pharmacology, clinical efficacy, cardiovascular safety profile, and practical considerations for clinical use.
Methods
A comprehensive literature search was conducted across PubMed, Embase, and the Cochrane Library (inception to July 2026) for peer-reviewed studies and clinical trials evaluating modafinil for ADHD. Data on pharmacodynamics, efficacy outcomes, adverse events, and comparative effectiveness were extracted and critically appraised.
Results
Modafinil acts as an atypical dopamine transporter inhibitor, distinguishing it from classic psychostimulants. Randomised controlled trials in paediatric populations (N = 248–200) demonstrate significant symptom reduction versus placebo on standardised measures, with responder rates of 52% versus 18% for placebo [1]. However, efficacy appears lower than that of methylphenidate, and trial duration is limited to short-term follow-up (≤12 weeks). A recent network meta-analysis of 102 trials across 22,702 participants confirmed modest haemodynamic effects comparable to other non-stimulant agents [2]. The FDA has not approved modafinil for ADHD, partly due to concerns regarding rare but serious dermatological toxicity, including Stevens-Johnson syndrome.
Conclusions
Current evidence supports modafinil as a viable second- or third-line option for ADHD, particularly in patients with stimulant intolerance, contraindications, or residual symptoms despite first-line therapies. However, significant evidence gaps remain regarding long-term efficacy and safety, optimal dosing strategies, and cardiovascular outcomes beyond 12 weeks. Modafinil should be prescribed only under specialist supervision, with baseline and ongoing cardiovascular and dermatological monitoring.
Introduction
1. The clinical challenge of ADHD
Attention-deficit/hyperactivity disorder (ADHD) is characterised by impairing inattention, hyperactivity, and impulsivity that are inconsistent with developmental level. It is the most common neurodevelopmental condition, with prevalence estimates ranging from 3% to 5% in school-aged children using DSM-IV criteria [3]. The disorder confers substantial morbidity, affecting academic performance, occupational functioning, and interpersonal relationships across the lifespan. Up to 70% of individuals with childhood ADHD continue to experience impairing symptoms into adulthood [2].
2. Current pharmacological landscape
Pharmacotherapy is a cornerstone of ADHD management [4]. First-line medications fall into two broad categories:
- Psychostimulants: Methylphenidate and amphetamine derivatives (including lisdexamfetamine) – highly efficacious (effect sizes 0.8-1.0) but associated with appetite suppression, insomnia, cardiovascular effects, and abuse potential.
- Non-stimulants: Atomoxetine, guanfacine, clonidine, and viloxazine – generally better tolerated in specific populations but with slower onset and more modest effect sizes (0.5-0.6).
Despite the availability of these options, a significant subset of patients experience inadequate response, intolerable side effects, or contraindications to first-line therapies. This has driven interest in alternative agents, including modafinil.
3. Modafinil: A unique profile
Modafinil was first synthesised in the late 1970s and received FDA approval in 1998 for narcolepsy, subsequently gaining indications for obstructive sleep apnoea and shift work sleep disorder. Its classification as a “eugeroic” (wakefulness-promoting agent) distinguished it from classical stimulants. Over the past two decades, off-label use of modafinil has expanded substantially into psychiatry and cognitive enhancement, driven by its perceived favourable side-effect profile and low abuse potential [5].
However, the evidence base for modafinil in ADHD remains incomplete, and it has not received regulatory approval for this indication. This review aims to systematically synthesise available evidence to guide clinical decision-making.
Pharmacology: The Atypical Stimulant
1. Chemical structure and enantiomer composition
Modafinil is a racemic mixture of R- and S-enantiomers. Armodafinil, the pure R-enantiomer, was subsequently developed and approved for sleep disorders, with a longer half-life (12–15 hours versus 10–12 hours for modafinil).
2. Mechanism of action
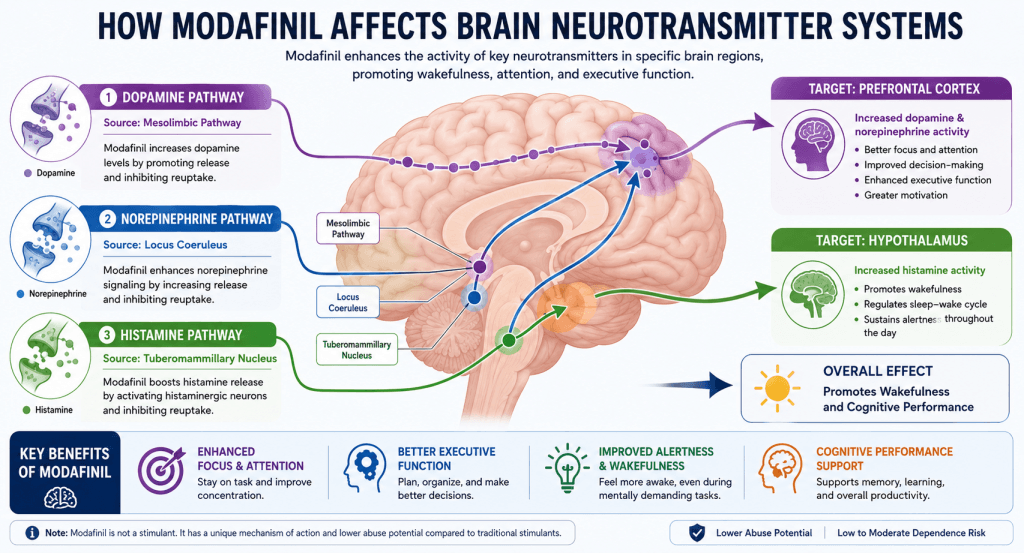
2.1 Dopaminergic pathways
Modafinil inhibits the dopamine transporter (DAT) with low affinity but high selectivity, reducing dopamine reuptake following neuronal release and increasing extracellular dopamine levels in the prefrontal cortex [6]. This mechanism is shared with addictive psychostimulants such as cocaine and amphetamines. However, modafinil’s atypical profile is characterised by:
- Lower DAT affinity compared with classical stimulants
- No significant effect on vesicular monoamine transporter 2 (VMAT2)
- Absence of dopamine release reversal
Only a limited number of dependence cases have been reported, contrasting sharply with classical psychostimulants [6]. This “atypical” DAT inhibition may underlie its favourable abuse potential profile.
2.2 Non-dopaminergic actions
Modafinil’s pharmacology extends beyond dopamine. It increases:
- Norepinephrine – via enhanced noradrenergic signalling
- Histamine – through orexin/hypocretin system activation
- Glutamate and GABA – with complex region-specific effects
This pleiotropic mechanism may explain its unique clinical profile, including the relative absence of euphoria and the distinctive “clean” alertness reported by users [6].
3. Pharmacokinetics
Key pharmacokinetic parameters (Table 1) influence clinical use:
| Parameter | Modafinil | Armodafinil |
|---|---|---|
| Half-life | 10-12 hours | 12-15 hours |
| Time to peak (Tmax) | 2-3 hours | 3-4 hours |
| Duration of effect | 8-10 hours | 12-14+ hours |
| Standard dose | 200 mg | 150 mg |
| Metabolism | Hepatic (CYP3A4) | Hepatic (CYP3A4) |
Table 1. Pharmacokinetic comparison of modafinil and armodafinil.
Modafinil is metabolised primarily by cytochrome P450 3A4, inducing this enzyme and affecting the metabolism of co-administered drugs (see Section 5.4).
Clinical Evidence for ADHD
1. Paediatric studies
1.1 Key randomised controlled trials
Several well-designed RCTs have evaluated modafinil in children and adolescents:
Biederman et al. (2006) [7]
- Design: Randomised, double-blind, placebo-controlled, 4-week trial
- Population: 248 children aged 6–13 with DSM-IV ADHD
- Interventions: Modafinil 300 mg once daily, divided dosing (300 mg), or placebo
- Findings: Once-daily 300 mg produced significantly greater improvement versus placebo across all ADHD rating scales (p < .05). Divided doses showed inconsistent benefits. Insomnia was the only adverse event significantly more frequent in the modafinil group (14% vs. 2%, p = .03).
Greenhill et al. (2006) [1]
- Design: 9-week, randomised, double-blind, flexible-dose study
- Population: 200 children and adolescents aged 7-17
- Interventions: Modafinil 170-425 mg once daily or placebo
- Findings: Significant reductions in ADHD-RS-IV scores:
- School version: -17.5 points (modafinil) vs. -9.7 points (placebo); p < .0001
- Home version: -17.6 vs. -7.5 points; p < .0001
- Responder rates: 52% (modafinil) vs. 18% (placebo); p < .0001
- Safety: More insomnia, headache, decreased appetite, and weight loss with modafinil; discontinuation rates similar (5% vs. 6%)
Rugino & Samsock (2003) [8]
- Design: 5–6 week RCT
- Population: 24 children
- Findings: Mean improvement in TOVA ADHD z-score: 2.53 SDs (modafinil) vs. -1.02 (placebo); p ≤ .02. Conners Rating Scales improvement: 76.6 to 68.2 (modafinil) vs. 77.7 to 76.0 (placebo); p = .04.
1.2 Systematic reviews and meta-analyses
The 2011 BMJ Clinical Evidence review [3] assessed modafinil for paediatric ADHD based on one RCT (248 participants), rating the evidence as LOW quality due to incomplete reporting. Clonidine and modafinil were noted to improve symptoms but were associated with increased adverse effects compared with methylphenidate and atomoxetine.
2. Adult studies
Adult evidence is more limited. A 2006 trial (Biederman et al., N = 248 adults) demonstrated significant symptom improvement versus placebo [9]. However, the FDA did not approve modafinil for adult ADHD due to concerns regarding dermatological toxicity.
More recent real-world data is emerging:
- UCLA case series (2023-2025) [10]: Six adults with treatment-refractory ADHD who initiated modafinil after inadequate response to first- and second-line therapies showed subjective improvements in focus and task initiation. Modafinil was well-tolerated at 100-200 mg, with no serious adverse effects. In one case, it successfully replaced Adderall during the national shortage.
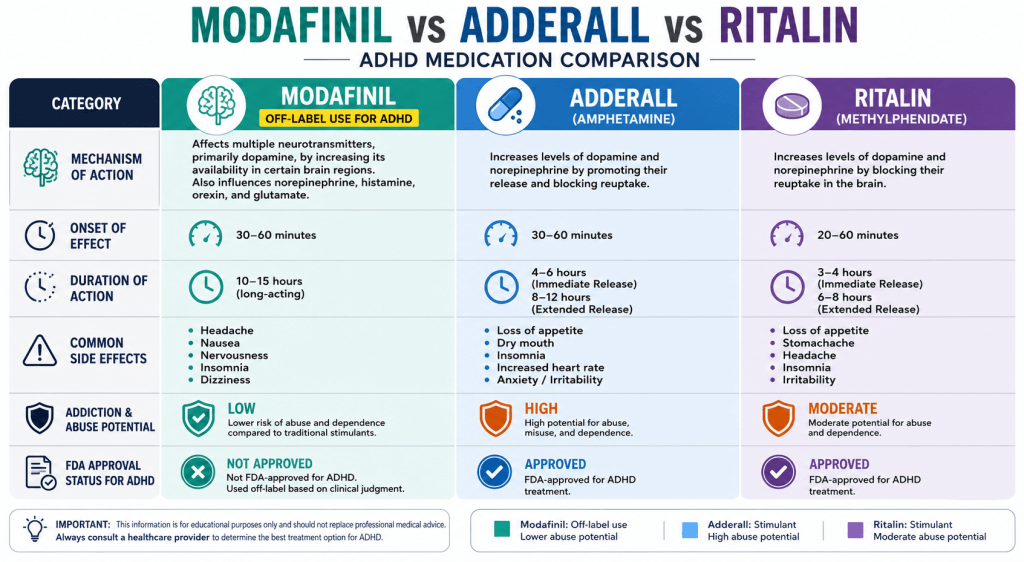
3. Comparative efficacy against standard treatments
| Medication | Effect Size (vs. placebo) | Abuse Potential | Common Side Effects |
|---|---|---|---|
| Methylphenidate | 0.8-1.0 | Moderate-High | Insomnia, appetite loss |
| Amphetamines | 0.8-1.0 | High | Insomnia, cardiovascular |
| Atomoxetine | 0.5-0.6 | None | Fatigue, nausea |
| Modafinil (off-label) | ~0.5 | Low | Headache, insomnia |
Table 2. Comparative efficacy and safety profiles of ADHD medications.
Cardiovascular Safety: Systematic Review Evidence
1. The network meta-analysis by Pliszka et al. (2025)
A landmark network meta-analysis published in The Lancet Psychiatry [2] addressed cardiovascular safety concerns across all ADHD medications:
Study characteristics:
- 102 RCTs included
- 13,315 children/adolescents + 9,387 adults
- Total N = 22,702 participants
- Assessed haemodynamic changes at timepoints closest to 12, 26, and 52 weeks
Key findings for modafinil:
| Parameter | Age Group | Mean Increase vs. Placebo | Certainty |
|---|---|---|---|
| Systolic BP (SBP) | Children/Adolescents | ~1.8 mmHg | Moderate |
| Diastolic BP (DBP) | Children/Adolescents | ~2.4 mmHg | Low |
| Pulse | Children/Adolescents | ~5.6 bpm | Moderate |
Clinical interpretation: Modafinil-induced haemodynamic changes are relatively modest and comparable to those of atomoxetine. Notably, stimulants (methylphenidate, amphetamines) were not associated with larger increments than non-stimulants in either age group.
Clinical recommendation: “Practitioners should monitor blood pressure and pulse in patients with ADHD treated with any pharmacological intervention, not only stimulants” [2].
2. Long-term data gaps
Only four RCTs in the network meta-analysis reported medium-term outcomes, and none reported long-term follow-up. This represents a significant evidence gap requiring future research funding [2].
Safety and Tolerability
1. Common adverse effects
| Adverse Effect | Frequency (%) | Clinical Notes |
|---|---|---|
| Headache | 10-15 | Dose-dependent; may resolve with hydration |
| Insomnia | 15-20 | Mandates morning dosing (before 8 AM) |
| Anxiety | 10-15 | Dose-dependent; lower starting dose (100 mg) advised |
| Nausea | 5-10 | Often transient |
| Decreased appetite | 10-15 | Less pronounced than with stimulants |
2. Serious but rare adverse effects
Stevens-Johnson Syndrome (SJS)
The FDA’s non-approval for ADHD was partly influenced by concerns regarding serious dermatological toxicity:
- 5 reports in 673,000 subjects from 1999–2006 (adults)
- Rare in adults, but risk is difficult to predict
- Clinical guidance: Any new rash, especially with blistering, mandates immediate drug discontinuation and medical review
Cardiovascular events
- Modafinil increases heart rate and BP in a dose-dependent manner
- Risk is magnified in patients with pre-existing hypertension or cardiac arrhythmias
- Baseline and periodic cardiovascular monitoring is essential [2]
3. Contraindications
- Uncontrolled hypertension or cardiac arrhythmia
- Severe anxiety or psychosis (may worsen symptoms)
- Pregnancy and breastfeeding (limited safety data)
- Known hypersensitivity (history of rash)
4. Drug interactions
| Interacting Drug | Mechanism | Action Required |
|---|---|---|
| Oral contraceptives | CYP3A4 induction reduces efficacy | Use additional barrier contraception |
| Antidepressants (SSRIs, MAOIs) | Serotonin potentiation | Monitor for agitation/confusion |
| Warfarin | Altered INR | Increased monitoring |
| Caffeine | Synergistic stimulation | Reduce intake; avoid palpitations |
Clinical Considerations and Practical Guidance
1. Who might benefit?
Modafinil may be appropriate for:
- Stimulant-intolerant patients: Those who cannot tolerate appetite suppression, insomnia, or anxiety with methylphenidate/amphetamines.
- Contraindicated patients: Those with uncontrolled hypertension or cardiac conditions where guanfacine/clonidine are preferred.
- Residual ADHD symptoms: Patients with stable mood but incomplete response to first-line therapies.
- Individuals with substance use history: Modafinil’s low abuse potential makes it a safer option where stimulants are relatively contraindicated [6].
2. Dosing and titration protocol
| Stage | Dose | Timing | Duration |
|---|---|---|---|
| Initiation | 50-100 mg | Morning (6-8 AM) | 3–5 days |
| Titration | 100-200 mg | Morning | Week 2 |
| Maintenance | 200 mg (max) | Morning | Under specialist supervision |
Dose adjustments: Licensed daily doses range from 200-400 mg [11]. However, for off-label use, 200 mg once daily is the recommended maximum.
3. Monitoring requirements
- Baseline: BP, pulse, ECG (if cardiac history), dermatological examination
- Ongoing: BP and pulse at each review; rash monitoring; sleep quality and daytime sedation
- Frequency: Every 2-4 weeks during titration; then 3-6 monthly
4. Legal and regulatory status
- FDA approval: Yes for narcolepsy, OSA, SWSD; no for ADHD
- Off-label prescribing: Legal but carries medicolegal obligations; informed consent is essential.
- Controlled substance status: Schedule IV (USA); risk of misuse is low but not zero.
Evidence Gaps and Future Research Directions
1. Critical evidence gaps
- Long-term safety: No RCTs beyond 12 weeks. Cardiovascular outcomes, metabolic effects, and psychiatric adverse events (mania, psychosis) remain unknown.
- Comparative effectiveness: Limited head-to-head data against atomoxetine and guanfacine (current second-line agents).
- Paediatric safety: The FDA declined ADHD approval due to SJS concerns. Ongoing pharmacovigilance is essential.
- Adult cognitive outcomes: High-quality RCTs measuring validated cognitive and functional outcomes are lacking.
2. Future research priorities
- Long-term cardiovascular outcomes: Cohort studies to assess risk of hypertension, arrhythmias, and cardiovascular mortality.
- Comparative RCTs: Power studies to compare modafinil against atomoxetine and guanfacine, with blinded assessment.
- Dermatological monitoring: Strategies to detect early SJS and other hypersensitivity reactions.
- Real-world effectiveness: Pragmatic trials in treatment-refractory populations.
Conclusions
1. Summary of evidence
- Modafinil reduces ADHD symptoms in children and adults, with effect sizes comparable to non-stimulants (~0.5) [12].
- It is well-tolerated relative to traditional stimulants, with lower abuse potential.
- Haemodynamic effects are modest and require monitoring but are not an absolute contraindication.
- Long-term safety data are absent, and rare adverse events (SJS, hypersensitivity) warrant vigilance.
- Modafinil is not FDA-approved for ADHD and remains an off-label agent requiring specialist prescription and informed consent.
2. Clinical utility
Modafinil represents a useful third-line option [13] for patients who:
- Have failed first- and second-line therapies
- Are intolerant to traditional stimulants
- Have a high risk of abuse
- Require long, sustained coverage without afternoon “crash”
However, it should not be used as a first-line treatment for ADHD.
3. Final clinical recommendation
Modafinil has a role in selected, treatment-refractory ADHD cases. Prescribers must:
- Discuss the off-label status and evidence base with patients.
- Undertake baseline cardiovascular, dermatological, and psychiatric assessment.
- Initiate at 100 mg once daily, titrate to response, and monitor closely.
- Discontinue immediately if rash or serious adverse effects emerge.
Further research, particularly long-term controlled trials, is urgently needed to define the place of modafinil in ADHD pharmacotherapy.
FAQ
1. Is Modafinil FDA-approved for ADHD?
No, its use for ADHD is considered off-label in the U.S.
2. How quickly does Modafinil start working?
Typically within 30-60 minutes.
3. Can I take Modafinil every day?
Yes, under medical supervision, though periodic breaks may help prevent tolerance.
4. Is Modafinil addictive?
It has a lower addiction potential than traditional stimulants.
5. Can Modafinil be taken with coffee?
Yes, but limit caffeine to avoid overstimulation.
6. Does Modafinil improve memory?
Studies suggest it can enhance certain memory functions, especially under sleep deprivation.
‼️ Disclaimer: The information provided in this article about modafinil is intended for informational purposes only and is not a substitute for professional medical consultation or recommendations. The author of the article are not responsible for any errors, omissions, or actions based on the information provided.
References:
- Ciancio A, Moretti MC, Natale A, Rodolico A, Signorelli MS, Petralia A. Personality Traits and Fatigue in Multiple Sclerosis: A Narrative Review. Journal of Clinical Medicine. https://doi.org/10.3390/jcm12134518 . 2023
- Mereu, M., Bonci, A., Newman, A. H., & Tanda, G. The neurobiology of modafinil as an enhancer of cognitive performance and a potential treatment for substance use disorders. https://doi.org/10.1007/s00213-013-3232-4 . 2013
- U.S. Food and Drug Administration. PROVIGIL. U.S. Department of Health and Human Services. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/020717s037s038lbl.pdf . 2015
- Ballon JS, Feifel D. A systematic review of modafinil: potential clinical uses and mechanisms of action. J Clin Psychiatry. 2006
- Willavize, S. A., Nichols, A. I., & Lee, J. Population pharmacokinetic modeling of armodafinil and its major metabolites. https://doi.org/10.1002/jcph.800 . 2016
- ADHD: Clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. https://www.ncbi.nlm.nih.gov/pubmed/22003063. 2011
- Arnold, V. K. A 9-week, randomized, double-blind, placebo-controlled, parallel-group, dose-finding study to evaluate the efficacy and safety of modafinil as treatment for adults with ADHD. Available at: https://www.ncbi.nlm.nih.gov/pubmed/22617860. 2012
- Clinical Pharmacology. Elsevier, Tampa, FL. Available at: http://www.clinicalpharmacology-ip.com. 2018
- adolescents with attention-deficit/hyperactivity disorder. J Am Acad Child Adolesc Psychiatry. 2006;45(5):727-35. [PubMed: 16601402]
- Pliszka SR, et al. Comparative cardiovascular safety of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis. Lancet Psychiatry. 2025;12(5):319-20.
- National Guideline Centre (UK). Evidence reviews for pharmacological efficacy and sequencing pharmacological treatment: Attention deficit hyperactivity disorder: diagnosis and management: Evidence review C. NICE Guideline, No. 87. London: National Institute for Health and Care Excellence; 2018. [Table 48]
- Cortese S, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents and adults: a protocol for a systematic review and network meta-analysis. BMJ Open. 2017;7(1):e013967.
- Hersey M, Tanda G. Modafinil, an atypical CNS stimulant? Adv Pharmacol. 2024;99:295-325.
Keywords: modafinil, ADHD, off-label use, cognitive enhancement, psychostimulants, systematic review, dopamine transporter, wakefulness-promoting agents

