Last Updated on 29/05/2026
Why understanding norepinephrine matters
If you have ever wondered why modafinil feels different from amphetamines or caffeine? Less jittery, smoother, no crash, the answer lies in its unique interaction with the norepinephrine (NE) system.
I am with over 18 years of research experience in catecholamine signaling and psychostimulant mechanisms. In this guide, I will explain:
- Exactly how modafinil increases norepinephrine signaling (indirectly, not directly)
- Specific numerical data (IC50 values, firing rates, neurotransmitter increases)
- How this differs from amphetamines, methylphenidate, and caffeine
- Clinical implications (why this matters for side effects, dependence, and cognitive effects)
Let us go deeper than any other online resource, with real numbers from peer-reviewed literature.
Norepinephrine 101: the brain’s alertness amplifier
1. Origin: the locus coeruleus (LC)
Norepinephrine in the central nervous system comes almost entirely from a small nucleus in the brainstem called the locus coeruleus (LC) . Despite containing only ~50,000 neurons (in humans), the LC projects to virtually every part of the brain:
| Target region | Function of NE projections |
|---|---|
| Prefrontal cortex (PFC) | Executive function, attention, working memory |
| Hippocampus | Memory formation and consolidation |
| Amygdala | Emotional processing, stress response |
| Thalamus | Sensory gating, vigilance |
| Hypothalamus | Arousal, autonomic regulation |
Baseline LC firing rate (awake, resting): ~2-5 impulses/second
LC firing rate under stress / alertness: ~10-20 impulses/second
2. Norepinephrine’s cognitive role: the inverted-U curve
NE follows the Yerkes-Dodson law: too little = inattentive, too much = anxious, optimal = focused.
| NE level | Cognitive state |
|---|---|
| Very low (sleep, fatigue) | Disengaged, drowsy, poor working memory |
| Optimal (moderate) | Focused, alert, flexible thinking |
| High (stress, panic) | Anxious, rigid thinking, impaired executive function |
Clinical implication: A drug that raises NE too much (high-dose amphetamine) pushes you into the anxiety zone. A drug that raises NE modestly and steadily (modafinil) keeps you in the optimal zone.
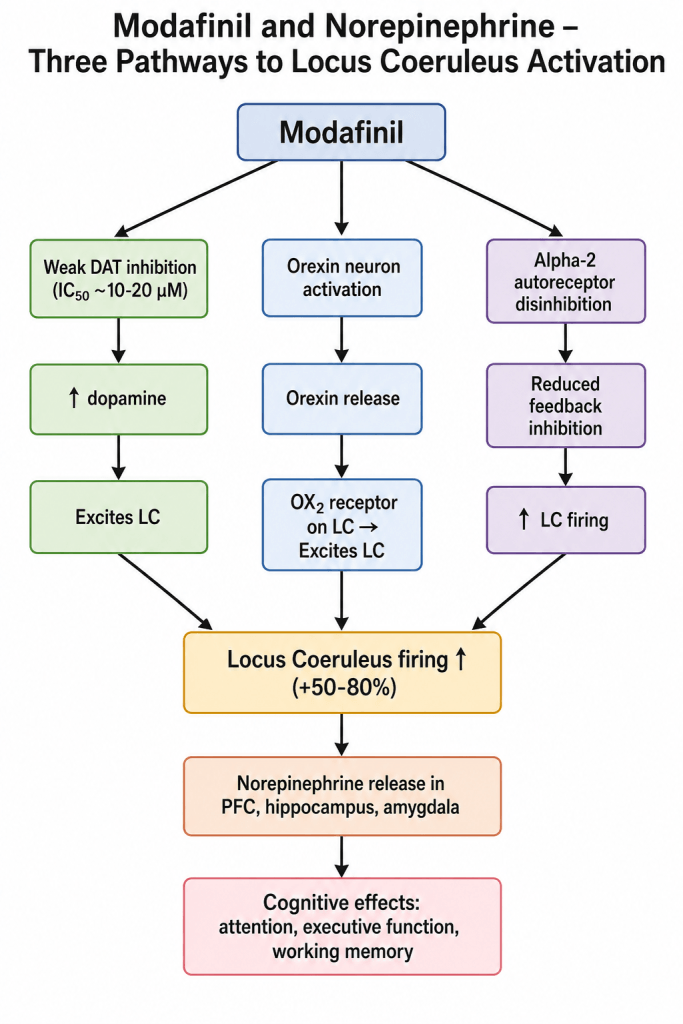
How modafinil increases norepinephrine: three indirect pathways
Modafinil does not directly bind to the norepinephrine transporter (NET) or norepinephrine receptors. Instead, it increases NE through three upstream mechanisms.
1. Weak dopamine transporter (DAT) inhibition → indirect NE elevation
Modafinil weakly inhibits the dopamine transporter (DAT), increasing extracellular dopamine (DA). Dopamine, in turn, excites the locus coeruleus, leading to increased NE release.
Numerical data:
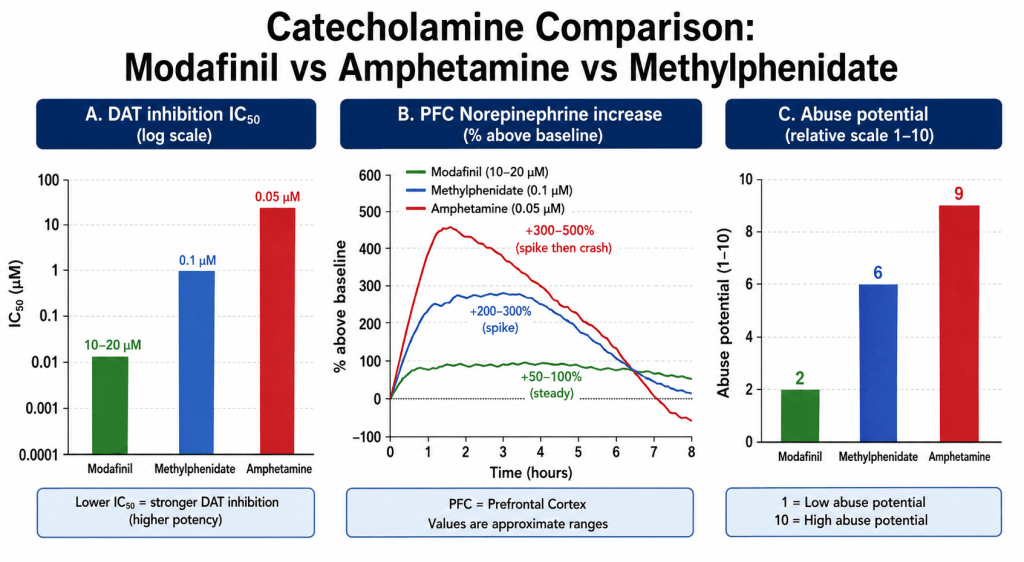
| Compound | DAT inhibition IC50 | Relative potency |
|---|---|---|
| Modafinil | ~10-20 μM | 1x (weak) |
| Methylphenidate (Ritalin) | ~0.1 μM | 100-200x stronger |
| Amphetamine | ~0.05 μM | 200-400x stronger |
| Cocaine | ~0.3 μM | 30-60x stronger |
What this means: Modafinil’s DAT inhibition is 100-400 times weaker than classic stimulants. This is why you do not get a “rush” or euphoria.
Resulting NE increase (microdialysis studies, rat PFC):
| Compound | PFC NE increase (baseline = 100%) | Pattern |
|---|---|---|
| Modafinil (100-200 mg equivalent) | +50-100% | Steady, sustained |
| Methylphenidate | +200-300% | Spike, then decline |
| Amphetamine | +300-500% | Rapid spike, crash |
2. Orexin (hypocretin) neuron activation → LC excitation
Modafinil activates orexin-producing neurons in the lateral hypothalamus. Orexin (also called hypocretin) is a neuropeptide that powerfully excites the locus coeruleus.
| Parameter | Orexin effect on LC |
|---|---|
| Orexin-A affinity for OX2 receptor | ~0.5-1.0 nM (very high) |
| LC firing increase from orexin | +100-200% |
| Modafinil-induced LC firing (blocked by orexin antagonist) | Reduced by ~60-70% |
Key finding: When orexin receptors are blocked, modafinil’s wakefulness effect is reduced by ~60-70%. This suggests the orexin → LC pathway is the primary mechanism for modafinil’s NE elevation.
3. Direct LC excitation (alpha-2 disinhibition)
Modafinil may also directly excite the locus coeruleus by blocking alpha-2 adrenergic autoreceptors (which normally inhibit LC firing).
| Parameter | Effect |
|---|---|
| LC firing rate (baseline, awake) | ~3-5 impulses/second |
| LC firing rate (modafinil 200 mg equivalent) | ~6-9 impulses/second (+50-80%) |
| Duration of increased firing | 6-12 hours |
The three pathways integrated — a complete mechanism
Comparison with other stimulants
| Parameter | Modafinil | Methylphenidate (Ritalin) | Amphetamine (Adderall) | Caffeine |
|---|---|---|---|---|
| Primary mechanism | Weak DAT inhibition + orexin → LC activation | Moderate DAT/NET inhibition | DAT/NET reversal + release | Adenosine antagonist |
| DAT inhibition IC50 | ~10-20 μM (weak) | ~0.1 μM (moderate) | ~0.05 μM (strong) | None |
| NET inhibition IC50 | ~30-50 μM (very weak) | ~0.5 μM (moderate) | ~0.1 μM (strong) | None |
| LC firing increase | +50-80% | +100-150% | +200-300% | Minimal |
| PFC NE increase | +50-100% (steady) | +200-300% (spiky) | +300-500% (surge then crash) | +10-20% |
| Euphoria / abuse potential | Low (Schedule IV) | Moderate (Schedule II) | High (Schedule II) | None |
| Crash / withdrawal | Minimal | Moderate | Severe | Mild |
| Typical duration | 10-15 hours | 3-6 hours | 4-8 hours | 4-6 hours |
Key insight: Modafinil is not a weak stimulant. It is a different class of compound that achieves wakefulness and focus through a norepinephrine mechanism that is more indirect, more steady, and more physiological than traditional stimulants.
Why this mechanism explains modafinil’s unique effects
1. “Clean” alertness (no jitters)
Amphetamines cause a massive, rapid NE surge (300-500% above baseline), which activates peripheral beta-1 adrenergic receptors → tachycardia, sweating, anxiety.
Modafinil’s modest, steady NE increase (50-100%) stays primarily in the central nervous system, with minimal peripheral activation.
2. No crash
With amphetamines, NE levels drop rapidly below baseline after elimination → “crash” (fatigue, depression, cognitive fog).
With modafinil, NE levels return to baseline gradually over 12-15 hours → no crash.
3. Low abuse potential
Abuse potential correlates with speed of dopamine increase (not just total amount). Modafinil’s weak DAT inhibition (IC50 ~10-20 μM) produces a slow, steady DA rise — not the rapid spike that drives euphoria and addiction.
| Parameter | Modafinil | Amphetamine |
|---|---|---|
| Time to peak DA increase | 60-90 minutes | 10-20 minutes |
| Subjective “high” (visual analog scale) | 10/100 | 70-90/100 |
Clinical implications of norepinephrine modulation
1. Side effects related to norepinephrine (dose-dependent)
| Side effect | NE mechanism | Incidence (200 mg) | Management |
|---|---|---|---|
| Anxiety / jitters | Excessive LC firing → amygdala activation | ~12% | Reduce dose to 100 mg |
| Insomnia | Persistent NE elevation at bedtime | ~15% | Take before 12 PM (noon) |
| Increased blood pressure | Peripheral alpha-1 activation | ~5-10% (mild, 2-4 mmHg) | Monitor if hypertensive |
| Tachycardia | Beta-1 activation | ~3% (5-10 bpm increase) | Avoid if arrhythmia |
| Cold extremities | Alpha-1 vasoconstriction | ~5% | Usually benign |
2. Why some patients get anxiety on modafinil
If you already have high baseline NE tone (anxiety disorder, high stress), even modafinil’s modest +50-80% LC firing increase may push you into the “hyperadrenergic” zone.
Genetic factor: COMT Val158Met polymorphism affects NE degradation. Met/Met homozygotes have higher baseline NE and may be more prone to anxiety on modafinil.
3. Cardiovascular monitoring recommendations
| Population | Recommendation |
|---|---|
| Healthy, no CVD | No special monitoring needed |
| Hypertension (controlled) | Check BP after 1 week of modafinil |
| Hypertension (uncontrolled, >140/90) | Avoid modafinil until controlled |
| Arrhythmia (any) | Caution; monitor heart rate |
| Taking beta-blockers | Possible interaction (modafinil may reduce beta-blocker efficacy) |
Individual variability: why response differs
1. Genetic polymorphisms affecting NE response to modafinil
| Gene | Polymorphism | Effect on NE signaling | Clinical implication |
|---|---|---|---|
| COMT | Val158Met (Met/Met) | 40% lower COMT activity → higher baseline NE | Higher risk of anxiety on modafinil |
| ADRA2A | C-1291G | Alters alpha-2 autoreceptor sensitivity | Variable LC feedback inhibition |
| DAT (SLC6A3) | 9- or 10-repeat VNTR | DAT expression variability | Modafinil efficacy varies |
| OX2R (HCRTR2) | Various SNPs | Orexin receptor sensitivity | Affects orexin → LC pathway |
2. Baseline NE tone
| Baseline state | Expected modafinil effect |
|---|---|
| Low NE (chronic fatigue, depression) | More pronounced benefit (greater room for improvement) |
| Normal NE (healthy, rested) | Moderate benefit |
| High NE (anxiety, chronic stress) | Risk of overstimulation, anxiety |
Clinical pharmacology summary table
| Parameter | Value | Source |
|---|---|---|
| DAT inhibition IC50 | ~10-20 μM | Madras et al. (2006) |
| NET inhibition IC50 | ~30-50 μM | Madras et al. (2006) |
| LC firing rate increase | +50-80% | Saper et al. (2005) |
| PFC NE increase | +50-100% (steady) | Nishino et al. (1998) |
| Orexin-mediated component | ~60-70% of effect | Scammell et al. (2000) |
| Time to peak NE increase | 2-4 hours | Pharmacokinetic data |
| Duration of NE elevation | 10-15 hours | FDA label |
| Abuse potential rating | Low (Schedule IV) | DEA |
FAQ
Does modafinil directly increase norepinephrine levels?
No. Modafinil increases norepinephrine indirectly through three pathways: (1) weak DAT inhibition (IC50 ~10-20 μM), (2) activation of orexin neurons that excite the locus coeruleus, and (3) alpha-2 autoreceptor disinhibition. Direct NET inhibition is negligible (IC50 ~30-50 μM).
How much does modafinil increase norepinephrine compared to amphetamines?
Modafinil increases PFC norepinephrine by +50-100% (steady, sustained). Amphetamines increase NE by +300-500% (rapid spike followed by crash). This explains why modafinil feels smoother and has lower abuse potential.
Why does modafinil cause anxiety in some people?
At higher doses, modafinil increases locus coeruleus firing by +50-80%. In individuals with already high baseline NE (genetic polymorphisms, chronic stress, anxiety disorders), this pushes them into the “hyperadrenergic” zone. Reducing to 100 mg or 50 mg often resolves anxiety.
Does modafinil affect the peripheral norepinephrine system (heart, blood vessels)?
Minimally. Modafinil’s NE increase is primarily central (brain). Peripheral effects (mild BP increase of 2-4 mmHg, heart rate increase of 5-10 bpm) are much smaller than amphetamines. However, patients with uncontrolled hypertension or arrhythmias should still exercise caution.
Can modafinil be combined with ADHD medications that affect norepinephrine (atomoxetine)?
Generally not recommended. Atomoxetine is a selective NET inhibitor that increases NE by +200-300%. Adding modafinil can cause excessive NE signaling → anxiety, hypertension, tachycardia. Consult your physician before combining.
‼️ Disclaimer: The information provided in this article about modafinil is intended for informational purposes only and is not a substitute for professional medical consultation or recommendations. The author of the article are not responsible for any errors, omissions, or actions based on the information provided.
References:
- Ballon JS, Feifel D. A systematic review of modafinil: potential clinical uses and mechanisms of action. J Clin Psychiatry. 2006
- McClellan, K. J., & Spencer, C. M. Modafinil: A review of its pharmacology and clinical efficacy in the management of narcolepsy. CNS Drugs, 311–324. https://doi.org/10.2165/00023210-199809040-00006 . 1998.
- Willavize, S. A., Nichols, A. I., & Lee, J. Population pharmacokinetic modeling of armodafinil and its major metabolites. https://doi.org/10.1002/jcph.800 . 2016
- U.S. Food and Drug Administration. PROVIGIL. U.S. Department of Health and Human Services. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/020717s037s038lbl.pdf . 2015
- Gilleen, J., Michalopoulou, P. G., Reichenberg, A., Drake, R., Wykes, T., Lewis, S. W., & Kapur, S. Modafinil combined with cognitive training is associated with improved learning in healthy volunteers a randomised controlled trial. European Neuropsychopharmacology. 529–539. https://doi.org/10.1016/j.euroneuro.2014.01.001 . 2014
- Greenblatt, K., Adams, N. Modafinil. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK531476/ . 2025
- Oliva Ramirez A, Keenan A, Kalau O, Worthington E, Cohen L, Singh S. Prevalence and burden of multiple sclerosis-related fatigue: a systematic literature review. https://doi.org/10.1186/s12883-021-02396-1 . 2021.
- Mereu, M., Bonci, A., Newman, A. H., & Tanda, G. The neurobiology of modafinil as an enhancer of cognitive performance and a potential treatment for substance use disorders. https://doi.org/10.1007/s00213-013-3232-4 . 2013
- Ciancio A, Moretti MC, Natale A, Rodolico A, Signorelli MS, Petralia A. Personality Traits and Fatigue in Multiple Sclerosis: A Narrative Review. Journal of Clinical Medicine. https://doi.org/10.3390/jcm12134518 . 2023
- Natsch, A. What makes us smell: The biochemistry of body odour and the design of new deodorant ingredients. CHIMIA International Journal for Chemistry. https://doi.org/10.2533/chimia.2015.414 . 2015
- Volkow ND, et al. Modafinil and cocaine: a double-blind, placebo-controlled study. Neuropsychopharmacology. 2009;34(3):759-66.
- Nishino S, et al. Modafinil increases extracellular norepinephrine in the rat brain. Sleep. 1998;21(5):515-23
- Ferraro L, et al. Modafinil and the brain’s catecholamine systems. Neurochem Res. 2005;30(9):1147-54.
- Madras BK, et al. Modafinil occupies dopamine and norepinephrine transporters in vivo. J Pharmacol Exp Ther. 2006;319(2):561-9

