
Last Updated on 01/07/2026
The high‑dose question I hear weekly
In my fourteen years as a community pharmacist, I’ve had hundreds of conversations about modafinil. But one question comes up more often than any other:
“If 200 mg makes me focused, shouldn’t 400 mg make me superhuman?”
The short, honest answer is no.
I’m not here to judge anyone. I’m here to give you the facts, the risks, and the context that many online forums gloss over. Whether you’re a student under pressure, a shift worker, or someone simply curious. This is the evidence‑based reality of taking 400 mg of modafinil.
What does the standard modafinil dosage look like?
Before we talk about high doses, let’s establish the baseline.
Recommended therapeutic range
According to the FDA‑approved prescribing information for Provigil (modafinil), the standard recommended dose is:
- 200 mg once daily: for narcolepsy and obstructive sleep apnea
- 200 mg once daily: for shift work sleep disorder (taken about 1 hour before shift)
Some patients start with 100 mg and increase to 200 mg if well tolerated.
What counts as a “high dose”?
In clinical practice and pharmacology:
- 200 mg = maximum standard dose
- 250–300 mg = elevated, sometimes used in clinical trials
- 400 mg = definitely high, used only in specific research settings or as a maximum safety limit
Anything above 200 mg is considered off‑label in terms of dosing. Meaning it hasn’t been rigorously tested or approved for routine use.
Why do some people consider taking 400 mg?
Understanding the motivation helps address the root of the question.
Common reasons I hear from patients and customers
- Tolerance frustration – “I’ve been on 200 mg for months, it’s not working like before.”
- The “more is better” fallacy – assuming a linear dose‑response curve.
- Competitive pressure – academic, financial, or professional environments where extreme focus feels necessary.
- Misreading online anecdotes – confusing “I took 400 mg and survived” with “400 mg is safe and effective.”
The tolerance trap
Tolerance to modafinil is real, but it’s not the same as with amphetamines. The drug’s effect on wakefulness is partly mediated by histamine and orexin pathways, which don’t downregulate as aggressively as dopamine receptors.
However, if you feel 200 mg isn’t working anymore, the clinically appropriate response is not to double the dose, it’s to take a drug holiday (2-3 days off) or consult your doctor to reassess the underlying condition. Chasing tolerance with escalating doses is a classic path to side effects, not to better outcomes.
The pharmacology behind 400 mg: what actually happens?
Let’s get scientific, but I’ll keep it practical.
Absorption and peak concentration
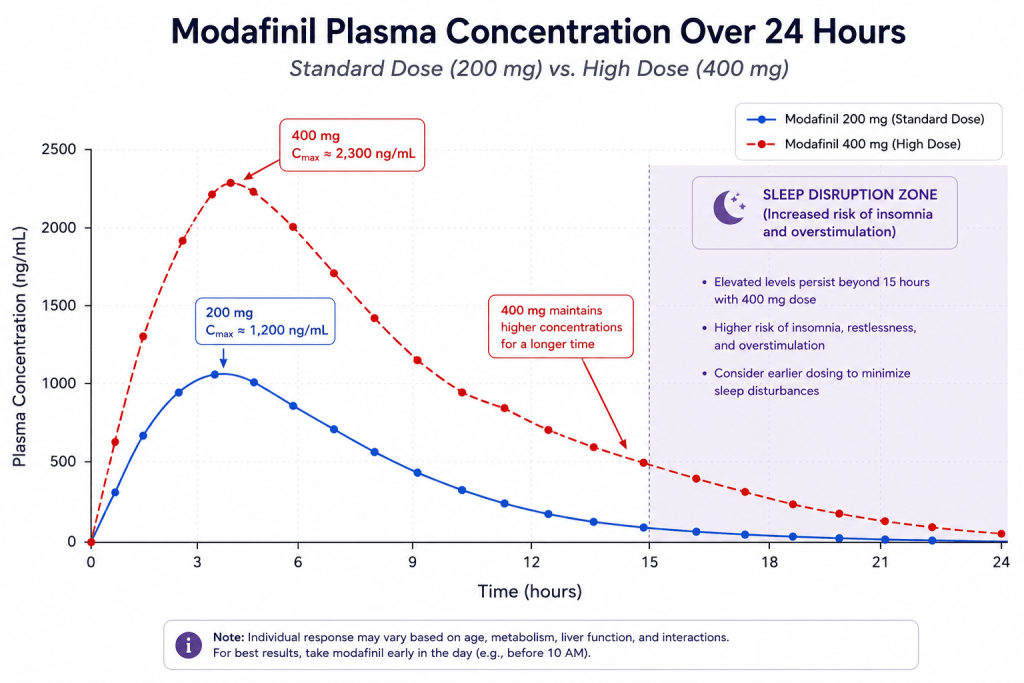
After oral administration, modafinil reaches peak plasma concentration (Cmax) in about 2-4 hours.
- 200 mg dose → Cmax approximately 4–5 µg/mL
- 400 mg dose → Cmax approximately 9–10 µg/mL
This means you get a much sharper spike, which increases the likelihood of:
- Headache
- Nausea
- Anxiety
- Jitteriness
Half‑life and accumulation
Modafinil has a half‑life of 12-15 hours in healthy adults.
With a 400 mg dose, the concentration remains above therapeutic threshold for much longer. Even 24 hours after ingestion, you still have significant amounts circulating. This directly translates to:
- Severe insomnia that night
- Fragmented sleep architecture (less deep sleep)
- Next‑day grogginess, paradoxically worsening your focus
Neurotransmitter effects
Modafinil increases dopamine, norepinephrine, and histamine. At 400 mg, this effect is amplified, but not in a linear, beneficial way.
High dopamine stimulation in the prefrontal cortex can improve working memory. But excessive stimulation in the amygdala and striatum can trigger:
- Over‑arousal
- Irritability
- Racing thoughts
- In extreme cases: panic attacks or transient paranoia
Is 400 mg of modafinil actually safe?
What the studies say
Several clinical trials have tested 400 mg doses, mainly to determine maximum tolerated limits or to explore efficacy in treatment‑resistant populations.
Key findings from published research:
| Study | Dose | Outcome |
|---|---|---|
| FDA clinical trials (Phase I) | 400 mg single dose | Well tolerated in healthy volunteers, but significantly higher adverse event rates |
| Long‑term narcolepsy studies | Up to 400 mg/day | Not superior to 200 mg for symptom control; more dropouts due to side effects |
| Cognitive enhancement trials | 300-400 mg | Minimal added benefit over 200 mg; increased anxiety and sleep disruption |
Takeaway: The scientific consensus is that 400 mg provides little to no additional benefit over 200 mg for most people, while substantially increasing the risk of adverse reactions.
Is it lethal?
No. The acute lethal dose of modafinil is very high: estimated above 1000 mg/kg in animal models. So a single 400 mg dose is not going to be fatal.
However, “not lethal” is a very low bar. The real questions are:
- Can it harm you in other ways? Yes.
- Can it cause serious complications in vulnerable individuals? Absolutely.
- Is it safe for you? That depends on your health status, genetics, and other medications.
Side effects at 400 mg
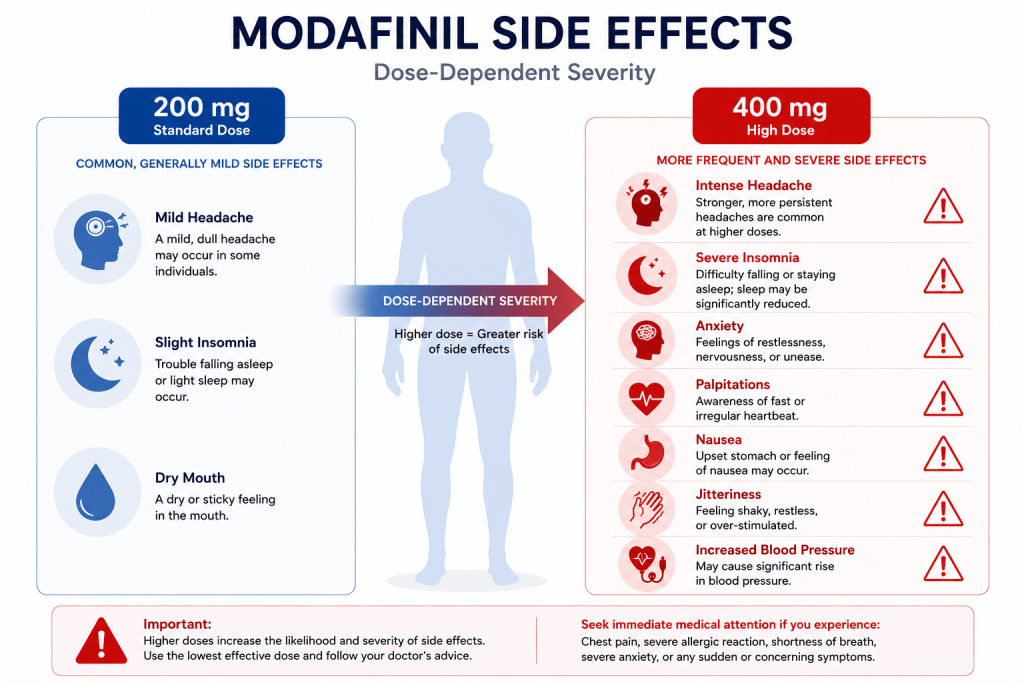
Based on clinical data and my own observations, here’s how side effect profiles compare.
| Side Effect | 200 mg (frequency) | 400 mg (frequency & intensity) |
|---|---|---|
| Headache | 10-15% | 35-50% more severe |
| Insomnia | 15-20% | 50-70% often prolonged |
| Nausea | 5-10% | 20-30% can be debilitating |
| Anxiety / jitteriness | 10% | 30-40% may require medical intervention |
| Palpitations | Rare | 5-10% concerning in cardiac patients |
| Blood pressure increase | Mild | Moderate, significant in hypertensive individuals |
| Skin reactions (rash) | Rare | Slightly increased risk |
Clinical pearl: The most common reason patients discontinue modafinil at high doses is not lack of efficacy, it’s intolerable side effects.
Short‑term and long‑term consequences of repeated 400 mg use
Short‑term (hours to days)
- Intense hyperfocus: but often inflexible, “tunnel vision” type
- Crash: when the drug wears off, fatigue can rebound severely
- Sleep deprivation: cumulative, even if you feel “fine”
Long‑term (weeks to months)
- Chronic sleep debt, linked to metabolic, immune, and cognitive deficits
- Psychological dependence, the belief you “can’t function” without it
- Potential liver enzyme induction, may affect metabolism of other drugs
- Worsening of underlying anxiety or bipolar disorder, not rare
I’ve seen patients who started at 200 mg, gradually increased to 400 mg over months, and eventually found themselves in a loop of poor sleep, higher doses, and diminishing returns. It’s a difficult cycle to break.
Who should absolutely avoid 400 mg?
This dose is contraindicated or at least very strongly not recommended in the following groups:
- Uncontrolled hypertension: risk of hypertensive crisis
- Cardiac arrhythmias: stimulant effect can provoke palpitations
- Anxiety or panic disorder: can precipitate severe episodes
- Psychiatric conditions: may worsen mania, psychosis, or agitation
- Liver impairment: modafinil is extensively metabolised by CYP3A4; high doses increase hepatic workload
- Pregnancy and breastfeeding: limited safety data; avoid unless explicitly prescribed by a specialist
- Elderly patients: slower clearance, higher sensitivity
- Patients on interacting medications
Dangerous drug interactions at high doses
At 400 mg, the risk of clinically significant interactions increases.
| Interacting drug | Effect |
|---|---|
| Oral contraceptives | Modafinil can reduce efficacy, high dose may lower hormone levels further |
| Antidepressants (SSRIs, MAOIs) | Increased serotonin stimulation, risk of agitation, serotonin syndrome |
| Caffeine | Synergistic stimulation: palpitations, anxiety, insomnia |
| Alcohol | Impaired metabolism, increased CNS depression and hangover effects |
| Anticoagulants (warfarin) | Possible altered INR, monitor more closely |
My advice: If you are on any prescription medication, never consider 400 mg without direct medical supervision and therapeutic drug monitoring.
Real‑world experiences
I always take online anecdotes with a grain of salt. But patterns are informative.
Positive reports
“Took 400 mg once for a 48‑hour deadline. I was incredibly focused, got everything done. But I couldn’t sleep for two nights and felt awful after.”
Negative reports
“400 mg made me so anxious I couldn’t type. My heart was racing. Definitely not doing that again.”
“I thought I could handle it because 200 mg was fine. Big mistake. I ended up with a headache that lasted all day and nausea.”
The most common theme: diminishing returns and amplified side effects.
Safe alternatives to high‑dose modafinil
If you feel 200 mg isn’t cutting it, consider these evidence‑based approaches before escalating.
1. Drug holidays
Take 1-2 days off per week. This helps reset receptor sensitivity and restores efficacy at the standard dose.
2. Stacking with non‑pharmacological strategies
- Sleep hygiene: 7-9 hours quality sleep improves baseline cognition
- Exercise: increases BDNF and improves executive function
- Hydration: even mild dehydration impairs focus
- Caffeine scheduling: limit to morning hours, avoid with modafinil
3. Lower doses, more frequently
Some patients do better with 100 mg twice daily (morning and early afternoon) rather than a single 200 mg. This maintains more stable plasma levels without the peak side effects.
4. Microdosing approach
A small subset of users report better subjective focus with 50 mg daily: less is sometimes more, especially for sensitive individuals.
5. Alternative nootropics (with proper caution)
If you are looking for cognitive support, consider:
- L‑theanine – gentle, promotes calm focus
- Rhodiola rosea – adaptogenic, supports mental stamina
- Lion’s mane mushroom – emerging evidence for cognitive health
These are not substitutes for modafinil in treating sleep disorders, but they may suit off‑label productivity goals with much lower risk profiles.
Legal and ethical context
Prescription requirements
In New Zealand, Australia, the UK, and the US, modafinil is a prescription‑only medicine. Obtaining it without a prescription is illegal.
The grey area of online sourcing
Many people buy modafinil online without a prescription. While enforcement varies, the risks are:
- Quality and purity issues (counterfeits)
- No medical oversight
- Customs seizure
- Legal consequences (rare for personal use, but possible)
Ethical reflection
I’m not here to preach. But I encourage you to ask yourself: Is a pill the most sustainable way to meet the pressure I’m facing? Often, the answer is more complex than pharmacology alone.
When to seek emergency medical help
Red flags after taking 400 mg
- Chest pain or palpitations – especially if radiating
- Shortness of breath
- Severe headache – unusual or thunderclap type
- Confusion, hallucinations, or paranoia
- Skin rash – especially if blistering or spreading (Stevens‑Johnson syndrome is rare but serious)
- Suicidal thoughts or severe agitation
What to do
- Stay calm – panic worsens symptoms.
- Hydrate – drink water slowly.
- Call your local poison information centre – they will guide you.
- If symptoms are moderate to severe, go to the nearest emergency department – take the medication packet or box with you.
FAQ
1. Can 400 mg of modafinil cause permanent damage?
Rarely from a single dose. Repeated high doses can contribute to chronic sleep deprivation, elevated blood pressure, and psychological dependence, but permanent organ damage is uncommon in healthy individuals.
2. Is 400 mg more effective than 200 mg for studying?
Clinical evidence says no. Most users report overstimulation, which actually impairs complex cognitive tasks like problem‑solving and creative thinking.
3. What if I already took 400 mg by mistake?
Don’t panic. Monitor your symptoms. Do not drive or operate machinery. Avoid caffeine and alcohol. If you feel unwell, seek medical advice.
4. Can I split a 400 mg tablet into two 200 mg doses?
Yes, but that defeats the purpose of asking about 400 mg. Splitting a 400 mg tablet gives you two standard doses which is fine.
5. How long does 400 mg stay in my system?
Given a 12-15 hour half‑life, it takes about 3-4 days to be completely eliminated (5 half‑lives). However, the stimulant effect lasts 12-18 hours.
Conclusion
To the question “Is it possible to take 400 mg of modafinil?” – the answer is yes.
To the more important question “Should you?” – almost certainly not.
The evidence, clinical experience, and pharmacology all point to the same conclusion: 400 mg provides no meaningful advantage over 200 mg for most people, and significantly increases the risk of adverse effects. It is not a shortcut to enhanced performance it’s a detour into side effects, sleep disruption, and unnecessary health risks.
My advice, as a pharmacist who has seen both the benefits and the downsides of this medication:
- Stick to the standard 200 mg dose.
- If it’s not working, talk to your doctor. Don’t self‑escalate.
- Support your brain with sleep, nutrition and exercise. They’re still the most reliable cognitive enhancers we have.
‼️ Disclaimer: The information provided in this article about modafinil is intended for informational purposes only and is not a substitute for professional medical consultation or recommendations. The author of the article are not responsible for any errors, omissions, or actions based on the information provided.
References:
- U.S. Food and Drug Administration. PROVIGIL. U.S. Department of Health and Human Services. https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/020717s037s038lbl.pdf . 2015
- Ballon JS, Feifel D. A systematic review of modafinil: potential clinical uses and mechanisms of action. J Clin Psychiatry. 2006
- Willavize, S. A., Nichols, A. I., & Lee, J. Population pharmacokinetic modeling of armodafinil and its major metabolites. https://doi.org/10.1002/jcph.800 . 2016
- Fuxe K, et al. Modafinil enhances the increase of extracellular serotonin levels induced by the antidepressant drugs fluoxetine and imipramine: a dual probe microdialysis study in awake rat. Synapse. 2005
- Mechanisms of modafinil: A review of current research. nih.gov. 2007
- PROVIGIL (modafinil) Tablets. FDA.GOV. 2010
- Oliva Ramirez A, Keenan A, Kalau O, Worthington E, Cohen L, Singh S. Prevalence and burden of multiple sclerosis-related fatigue: a systematic literature review. 2021.
- Ciancio A, Moretti MC, Natale A, Rodolico A, Signorelli MS, Petralia A. Personality Traits and Fatigue in Multiple Sclerosis: A Narrative Review. Journal of Clinical Medicine. 2023
- Mereu, M., Bonci, A., Newman, A. H., & Tanda, G. The neurobiology of modafinil as an enhancer of cognitive performance and a potential treatment for substance use disorders. https://doi.org/10.1007/s00213-013-3232-4 . 2013
- Woo, J., & Verduzco-Gutierrez, M. Traumatic brain injury: An overview of epidemiology, pathophysiology, and medical management. Medical Clinics of North America. https://doi.org/10.1016/j.mcna.2019.11.001 . 2020
- Oliva Ramirez A, Keenan A, Kalau O, Worthington E, Cohen L, Singh S. Prevalence and burden of multiple sclerosis-related fatigue: a systematic literature review. https://doi.org/10.1186/s12883-021-02396-1 . 2021

